
Child Malnutrition in Cambodia

Photo by bag_lady on Flickr

By Ashley Girvin Bernal
Published Fall 2022
Special thanks to Seth Ririe for editing and research contributions.
Summary+
Malnutrition has been recognized as a global issue and has a high prevalence in poorer countries like Cambodia. Children are most affected by malnutrition, especially those under age 5. Malnourished children are at an increased risk for developing diseases, developmental delays, and dying at an earlier age. Child malnutrition in Cambodia is primarily due to a lack of education, cultural beliefs and practices, food insecurity, and recurrent diarrhea. The current best practice is vitamin A supplementation, provided by groups such as Helen Keller International through medical professionals and community volunteers.
Key Takeaways+
- Every year malnutrition causes over half of child deaths worldwide, and as of 2016, 4,454 children die in Cambodia annually because of malnutrition.228, 229
- In 2019, 32% of children under 5 in Cambodia were stunted, 10% were wasted, and 24% were underweight.230
- In Cambodia, more than 60% of children aged 12 to 23.9 months and up to 80% of children aged 6 to 8 months do not receive the minimum acceptable daily diet.231
- The average amount of time mothers spent breastfeeding was 2 months, while the longest any mother reported breastfeeding her child was for 4 months.232
- In children under age 5, 53% of deaths due to diarrhea were also related to malnutrition.233
- Vitamin A supplementation reduced diarrheal occurrences by 40% and mortality by 23% in children aged 6 months to 5 years in Cambodia.234
Key Terms+
Anemia—A medical condition that occurs when you do not have an adequate supply of healthy red blood cells to carry enough oxygen throughout the body.1
Colostrum—The first form of breastmilk produced in the first days after an infant is born. It is high in nutrients, as well as antibodies and antioxidants. Colostrum changes to regular breast milk within 2 to 4 days of birth.2
Energy Intake—Refers to the total amount of energy consumed through dietary sources, such as carbohydrates, proteins, and fats.3
Enteric Pathogens—Bacterias in the intestines of humans and animals that cause diseases.4
Essential Nutrients—Nutrients that can only be received through consumption.5
Macronutrients—Nutrients that the body uses in large amounts, such as carbohydrates, proteins, and fat.6
Micronutrients—Vitamins and minerals that the body requires in small amounts and are critical to health. Micronutrient deficiencies can cause a reduction in energy level and mental clarity as well as severe and fatal conditions.7
Morbidity—Having a disease or symptoms of the disease. It can also refer to the amount of a disease within a population. Morbidity also includes medical problems that were caused by a treatment.8
Mortality—Refers to death or the death of large numbers of people.9
Neonatal—A term referring to newborns, particularly during the first month of life.10
Stunting—Refers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12
Wasting—When children have a low weight-for-height ratio. Wasting indicates malnutrition; children that are wasted have a higher risk of dying from common diseases.13
Context
Q: What is Malnutrition?
A: Malnutrition refers to nutrient deficiencies or excesses, impaired nutrient utilization caused by the lack of proper food intake, or an imbalance of said nutrients.14 There are four main types of malnutrition that are common in developing countries: protein-energy malnutrition (PEM), iron deficiency, vitamin A deficiencies (VAD), and iodine deficiencies.15 The World Health Organization refers to malnutrition as a “double burden” because it includes both cases of undernutrition and those of obesity, overnutrition, and other diet-related diseases.16 While all forms of malnutrition are worth addressing, this brief will primarily focus on undernutrition because overnutrition and obesity account for less than 2% of the population in Cambodia.17 Undernutrition occurs when a person does not consume the necessary nutrients for healthy growth and development. The generally-accepted main indicators of undernutrition are individuals who are underweight, stunted, or wasted. Underweight refers to low weight for age, wastingWhen children have a low weight-for-height ratio. Wasting indicates malnutrition; children that are wasted have a higher risk of dying from common diseases.13 to low weight for height, and stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12 to low height for age. This brief will use these indicators to measure undernutrition in Cambodia.
Essential nutrientsNutrients that can only be received through consumption.5 are nutrients that are vital for growth but must be consumed due to the body's inability to produce them.18 Of the 20 amino acids in protein, 8 are considered essential. Certain minerals can also be classified as essential, including calcium, magnesium, iron, iodine, and zinc.19 Vitamin A, one of the most important nutrients for healthy growth and development, supports immune function, cellular communication, the reproductive systems, vision, and cell growth and differentiation, particularly regarding the formation and maintenance of the heart, lungs, eyes, and other organs.20, 21
Q: What does healthy growth and development look like, and what nutrients does it require?
A: Growth refers to a physical increase in the body or its parts, while development deals with functional changes that result from emotional and social interactions.22 This means that healthy growth in a child is defined as when a child does not show signs of illness and grows steadily both physically and physiologically; healthy growth and development also account for good cognitive development.23 When children are affected by malnutrition, all forms of growth and development suffer.
Basic nutrient requirements include both macronutrientsNutrients that the body uses in large amounts, such as carbohydrates, proteins, and fat.6 and micronutrientsVitamins and minerals that the body requires in small amounts and are critical to health. Micronutrient deficiencies can cause a reduction in energy level and mental clarity as well as severe and fatal conditions.7. The recommended energy intakeRefers to the total amount of energy consumed through dietary sources, such as carbohydrates, proteins, and fats.3 distribution includes 15% from proteins, 40–50% from lipids (fats), and 40–55% from carbohydrates.24 Infants also require the following micronutrientsVitamins and minerals that the body requires in small amounts and are critical to health. Micronutrient deficiencies can cause a reduction in energy level and mental clarity as well as severe and fatal conditions.7: iron, zinc, copper, chromium, manganese, selenium, and Vitamins A, B, C, D, E, and K.25 Plants should form part of a healthy diet because they contain many nutrients—such as vitamins A and C—and they often contain minerals and proteins.26 Infants and children require larger amounts of vitamin A to support rapid growth and to aid in combating infections.27 Unlike adults, whose diets mostly work to maintain health, children’s diets should seek to support healthy growth and development.28
In order to achieve healthy growth and development, a child must consume a wide variety of foods from different food groups, which together contain many essential nutrientsNutrients that can only be received through consumption.5 and adequate energy, fat, and protein. As mentioned previously, one of the most vital nutrients is vitamin A.29 Iron is another nutrient that is important to growth and development because it is part of red blood cells that transport oxygen throughout the body. It is also important for physical growth, neurological development, and cellular functioning.30, 31, 32 Iodine is also necessary for growth and is often deficient in developing countries. Iodine is a vital component of the thyroid hormones, which helps regulate protein synthesis, enzymatic activity, and metabolic activity.33 In fetuses and infants, iodine serves to develop proper skeletal and central nervous systems.34, 35 Zinc is another micronutrient that is important for growth, cognitive development, and wound healing.36 Thiamine is also important for consumption because its function is the growth, development, and function of cells.37 The recommended daily intake of each of these nutrients, along with foods associated with them, are listed in this paragraph's accompanying graphic.


Q: What does malnutrition look like in Cambodia, and what areas are impacted the most?
A: Data from the World Health Organization shows that in 2020, 22% of children worldwide (484 million) experienced stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12, while less than 1% of children (13.6 million) experienced wastingWhen children have a low weight-for-height ratio. Wasting indicates malnutrition; children that are wasted have a higher risk of dying from common diseases.13.38, 39 A recent publication showed that in southeast Asia, 29.4%, 18.3%, and 9.4% of all children under 5 were stunted, underweight, and wasted, respectively.40 These rates amount to approximately 15.6 million children who were stunted, 9.7 million who were underweight, and 5 million who were wasted.41 In Cambodia, indicators of undernutrition were higher than both Southeast Asia and worldwide averages, as 32% of Cambodian children under 5 were stunted, 24% were underweight, and 10% were wasted.42 In Cambodia, stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12 is considered of high to very high significance and wasting of medium to high significance (based on both indicators from the World Health Organization and the prevalence of child stunting and wastingWhen children have a low weight-for-height ratio. Wasting indicates malnutrition; children that are wasted have a higher risk of dying from common diseases.13 in Cambodia).43 Out of the population, only 21–28% of Cambodians receive the recommended intake of 2,100 calories per day (more than one-third of the population eat less than 2,100 calories), making Cambodia the country with the highest malnutrition rates in Southeast Asia.44, 45, 46 Only 19% of those who consume the recommended daily caloric intake consume the daily recommended iron intake, and only 27% of these individuals consume the daily recommended vitamin A intake.47 The number of stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12 cases varies by region, but families in rural areas are more at risk for malnutrition. These rural families comprise nearly 85% of the population.48 For instance, Phnom Penh is the largest city in Cambodia and resides in the Southern part of the country. There, 18% of children are stunted. In both Preah Vihear, a rural province of Cambodia that shares a border with Thailand, and Stung Treng, a rural northeast province that shares a border with Laos, 44% of children are stunted.49 Cases of malnutrition are more prevalent in rural areas where poverty is more significant.
Q: Who in Cambodia is most affected by malnutrition?
A: Research indicates that around 33% of the total Cambodian population is malnourished, meaning that more than one-third of the population does not meet the recommended daily calorie and nutrient intake.50 However, women and children are disproportionately affected by malnutrition because children need nutrients to grow and develop, and women need an increased amount of nutrients for themselves and their fetuses during pregnancy. In Cambodia, 10% of children under age 5 are wasted, and 32% are stunted.51 A study done in 2010 showed that 19% of non-pregnant women between 14–49 years old were underweight.52 A more recent study found that 21.4% of pregnant women had poor nutritional status and that 14.4% of the women living in urban areas were underweight.53 Even though malnutrition affects people of all ages in Cambodia, this brief will focus on undernutrition in children under age 5.

Photo by bag_lady on Flickr
Q: How does malnutrition in Cambodia affect children?
A: The recommended adequate diet varies by age, size, and gender. According to the US Department of Health and Human Services, males between 1–3 months need to consume between 472–572 calories per day, while females of the same age need to consume between 438–521 calories per day.54 This amount increases with age; at 12 months, recommended consumption reaches between 793–844 calories per day for males and 717–768 calories per day for females. By 2–3 years of age, both male and female children should consume between 1,000–1,400 calories per day, depending on activity level.55 Research done in three different Cambodian provinces on preschool children showed that the least amount of calories consumed by a preschooler was 775.9 kilocalories (kcal), and the highest amount consumed was 922.9 kcal.56 The study showed that only 30% of preschoolers consumed the recommended dietary intake for energy (calories).57
In Cambodia, more than 60% of children aged 12–23.9 months and up to 80% of children aged 6–8 months did not receive their minimum acceptable daily diet.58 Infants are recommended to consume a milk-based diet until at least 6 months of age, when they can then transition to semi-solid foods.59 One study indicates that 56% of infants in Cambodia aged 6 months and younger were breastfed the minimum recommended amount (6 times per day). Another study concluded that inadequate breastfeeding practices and complementary feeding practices that do not meet the minimum acceptable daily diet left children at higher risk of malnutrition during the early stages of life.60 If children do not drink enough breastmilk, they are not getting all the nutrients and calories their bodies need. Between ages 2–5, it is important for a child to consume plenty of proteins, fatty acids, and micronutrientsVitamins and minerals that the body requires in small amounts and are critical to health. Micronutrient deficiencies can cause a reduction in energy level and mental clarity as well as severe and fatal conditions.7 to meet their energy requirements.61 In Cambodia, 7.9% of children under 5 had a folate deficiency. Folate is important for DNA synthesis and amino acid metabolism, as well as neural tube defects during fetal development.62 Also, 22.3% of children under 5 are vitamin A deficient, and 15% are thiamine deficient.63 In Cambodia, more than 60% of reproductive-age women and children under 5 were zinc deficient, and 67.5% of preschool-age children had zinc deficiencies. Sixty percent of mothers and children were found to be deficient in iodine, with those living in rural areas being the most affected.64 The inability to provide adequate nutrition to younger children, specifically those under age 5, has directly impacted their growth and micronutrient status.65 Undernutrition in children under age 5 is of particular concern because children grow more during the first 5 years of life than in subsequent years.66
Q: How long has child malnutrition affected Cambodia?
A: Before the 1970s, Cambodia’s natural food resources prevented severe famine and mass starvation.67 However, between April 1975 and January 1979, about 1.5 million Cambodians died of malnutrition, overwork, and disease due to the policies and practices of the Khmer Rouge, a radical communist movement that ruled Cambodia during that time. This period was the most severe famine in modern Cambodian history.68 As part of their efforts to increase communism, the government forced many Cambodian citizens to farm.69
One of the first orders of the Khmer Rouge was to evacuate the capital city of Phnom Penh and send its citizens to farm the countryside. The leaders wanted to produce 3 tons of rice per hectare (2.47 acres), almost triple the amount previously produced, which would require forced labor of the citizens from sunrise to sunset and without the help of modern farming technologies.70 This hard labor caused Cambodians to burn more calories faster. The Khmer Rouge then focused on establishing communal meals and forbade any foraging for food or private gardens.71 Citizens needed even more nourishment after working all day in the fields but were unable to receive the nutrients they needed due to these food-related policies.72 The leaders of the Khmer Rouge also closed Cambodia off to the world market and banned the ability of citizens to feed themselves aside from government rations. Many citizens starved and became malnourished due to insufficient rations and a lack of necessary nutrients while their leaders ate what came from the harvests.73 Even though the Khmer Rouge only retained power until 1979, it greatly impacted the Cambodian population and economy. Many citizens are still experiencing the consequences of the movement through the loss of family members, a damaged economy, and illness, including malnutrition.74
Since the fall of the Khmer Rouge in 1979, researchers have been focusing on malnutrition and child mortalityRefers to death or the death of large numbers of people.9 rates in Cambodia.75 According to one study, surveys in 1992, 1997, 2002, and 2006 tracked changes in malnourishment cases within the population. The study concluded that even though there have been improvements in Cambodia with fewer cases of malnutrition, there are still a significant number of cases.76 As previously mentioned, in 2019, the prevalence of stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12, wasting, and underweight children sat at 32%, 10%, and 24%, respectively, for children under 5 in Cambodia.77 Further improvements in food security, income, education, health, and infrastructure would be beneficial to the country.78
Q: What is a typical diet in Cambodia?
A: The typical Cambodian diet consists of rice, soup, sweet stew, and fish. Cambodians use soy sauce, fish sauce, and salt as condiments. They live a communal lifestyle and normally eat food together as a family.79 Their diets tend to lack sufficient meat, vegetables, and fruit. Snacks high in fats, sugar, and salt are commonly eaten by Cambodian children.80 Additionally, vegetable production is limited and varies by season, thereby lessening the practice of growing and consuming vegetables that are high in essential nutrientsNutrients that can only be received through consumption.5. Cambodians typically eat less than 50% of the recommended daily intake of vegetables.81
Contributing Factors
Lack of Education
The lack of education within the Cambodian community has a direct impact on the health of their children. The level of education is affected by socioeconomic class, with the wealthy having more access to education than the poor. One source found that among the highest class, only 19% of children are stunted, but among the lowest class, 42% of children were stunted.82 Many of these children cannot attend school because their families cannot cover the cost of attendance. This lack of education causes children not to learn important nutritional information in school and not to receive food supplements (sometimes provided by non-government organizations at schools) to aid in their development.83 In a randomized control trial done in 2012, consequences of malnutrition were more prevalent in children who had mothers with no education.84
One survey found that in the northeastern region of Cambodia, 30% of children who had mothers with no education were stunted.85 Another study concluded that maternal education has an effect on stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12 and found that 27% of children who had mothers with secondary education were stunted, while 39% of children with mothers who had no formal education were stunted.86 The results of these studies could be because part of the general education school curriculum of Cambodia includes a focus on hygiene, health, and food.87

Lack of education leads to undernutrition because, without education, parents may not fully understand the importance of healthy eating and are unaware of which foods and what quantity of foods contain the nutrients that their children need for healthy growth and development.88 One example of this issue is that, on many occasions, the mother is unaware of the nutritional needs of a newborn child and thus waits to begin breastfeeding the child until 2 or 3 days after birth.89 In 2014, one survey showed that the number of infants receiving feedings before breastfeeding went from 19.1% to 27.7%90 Infants who are given pre-lacteal feedings lose the benefits of colostrumThe first form of breastmilk produced in the first days after an infant is born. It is high in nutrients, as well as antibodies and antioxidants. Colostrum changes to regular breast milk within 2 to 4 days of birth.2 which is nutrient-dense and high in antioxidants and antibodies that help build the newborn’s immune system.91, 92 When not breastfed within the first few days of life, infants lose those benefits and are 3.9 times more likely to later take breastmilk substitutes rather than breastmilk.93 Parents could be aware that breastfeeding is recommended, but because they do not understand why it is unlikely to be put into practice.94
Many parents know that pregnant women need to have visits with their doctors multiple times and to eat healthy foods, but they do not know what constitutes healthy eating, how much to eat, and the importance of gaining weight during pregnancy.95 One study concluded that this could be due to the lack of proper nutrition counseling during antenatal care visits at health centers.96 Many Cambodian mothers are not aware of the nutritional needs of their children because they have not been properly taught or they believe that what they are feeding their children is sufficient, which is further explained in the next contributing factor section.97 A focus group done in Cambodia showed that women with previous nutrition education were better able to identify treatments for a variety of symptoms that are common in nutrient deficiencies.98 Women who had no previous nutrition education were able to identify a vitamin A deficiency but were unable to identify specific treatments for deficiencies, rather stating that they needed to eat healthier or use traditional medicines.99
Nutrition education is particularly important in the first 2 years of a child’s life. The child grows and develops a significant amount during that time, and if they are not well nourished, they could develop stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12 or wastingWhen children have a low weight-for-height ratio. Wasting indicates malnutrition; children that are wasted have a higher risk of dying from common diseases.13 at an earlier age and have a higher risk of malnutrition-related complications.100 Nutrition education is especially important for pregnant women, who are the key determinants as to whether or not a child is born malnourished. When pregnant women do not eat nutrient-rich foods or a wide variety of foods during pregnancy, the infant is also affected.101 For an infant to experience healthy growth and development, they need to meet basic nutrient requirements; they cannot meet those requirements if their caregiver does not receive an education or cannot care for themself nutritionally.102 One source published in 2018 states that in Cambodia, more than 70% of children were not meeting these minimum daily requirements.103
Cultural Beliefs and Practices
Different cultural beliefs and practices cause malnutrition rates to rise as individuals remove necessary nutrients during food preparation and limit their diet. Most sources indicate that these practices are common and traditional, but specific numbers of how many people follow these practices in Cambodia are unavailable. One of these practices is that women at the childbearing stage change their eating habits to avoid “hot foods,” which results in a loss of nutritional diversity.104 This belief towards hot foods stems from Buddhist beliefs in Cambodia that indicate that eating hot foods will make the baby too hot.105 This is because they believe that pregnancy is a “hot state,” so eating hot foods during pregnancy is harmful to the mother and could result in an unwanted abortion.106 These Buddhist practices are followed by about 95% of the Cambodian population.107 Regarding the consumption of hot foods during pregnancy, women specifically avoid consuming warm water, hot ginger and jasmine tea, hot pork, fish or chicken, jasmine rice, black pepper, and ginger. Instead, they consume “cold foods,” such as cold water, juice, and raw fruits and vegetables as available, and commence eating hot foods again 6 weeks postpartum, which is believed to be important for the health of both the mother and the child.108 It is believed that not following the hot/cold schedule could result in maternal illness and unsuitable breast milk that will affect the child’s well-being.109 By removing hot foods from the diet, a pregnant woman loses nutrient diversity (specifically protein-rich foods from animal-based proteins) which are essential for the growth and development of the fetus. By not consuming animal proteins, which are considered “hot foods,” pregnant women lose access to many important nutrients, including proteins, fats, iron, iodine, calcium, vitamins A and D, and folate.110
Cambodian women also reduce their food intake in the hopes of having a smaller fetus and an easier delivery.111 Many pregnant women also choose to forego buying healthy, nutrient-rich foods in order to save more money for the delivery, which can cost between $10.00–250.00 for an overnight stay, $60.00 for a vaginal birth, and $278.00 for a c-section112, 113 These dollar amounts are significant because 18.6% of the population makes only $1.25 per day, making it difficult for many Cambodians to save for birth-giving while also purchasing nutrient-rich foods.114 Cambodian women typically recognize the need to increase consumption, but they tend to only increase consumption of routine foods such as rice rather than consuming more foods with higher levels of protein and micronutrientsVitamins and minerals that the body requires in small amounts and are critical to health. Micronutrient deficiencies can cause a reduction in energy level and mental clarity as well as severe and fatal conditions.7.115 While pregnant and breastfeeding, many women avoid consuming fish paste, a food that is high in essential nutrientsNutrients that can only be received through consumption.5, easily accessible in the region, and that is normally used daily as a condiment.116 They avoid fish paste and other fish products because of the way it negatively affects the smell of breastmilk.117 Other animal products are also avoided, especially when dealing with blood or internal organs of the animals because they are considered hot foods.118, 119 As discussed before, breastfeeding is not a common practice in Cambodia. As well as a lack of education, this can be attributed to cultural beliefs and practices. Instead of breastfeeding, newborns are given water, sugar water, or honey.120 One source states that the mothers waited a few days to breastfeed so as not to feed the baby colostrumThe first form of breastmilk produced in the first days after an infant is born. It is high in nutrients, as well as antibodies and antioxidants. Colostrum changes to regular breast milk within 2 to 4 days of birth.2, but the source did not indicate why the mothers wanted to avoid colostrum. After beginning to breastfeed, the mothers would still give the infants sugar water, honey, and other supplements to finish the feeding session.121 One study surveying 5,172 children found that in Cambodia, the average time mothers spent breastfeeding was 2 months. The longest any mother reported breastfeeding her child was for 4 months.122 However, the WHO recommends exclusive breastfeeding for infants up to 6 months of age.
After 6 months, infants should receive both nutritious foods and breast milk.123 Eating sufficient nutrient-rich foods during pregnancy and breastfeeding, as well as exclusive breastfeeding after birth, is important for the development of the fetus and newborn child.124 Neglecting positive practices leads to child undernutrition beginning with conception and continuing during infancy and adolescence.125

Photo by Feed My Starving Children on Flickr
For a child to be properly nourished, they must receive enough nutrients and various nutrients. A common belief in Cambodia is that if a child is gaining weight, they are receiving proper nutrients.126 Research shows that most Cambodian people consider rice nutritious enough to support healthy weight gain in children. The exact number of Cambodians that this applies to is not available. This belief influences widespread inadequacies of feeding practices.127 However, even if a child gains weight, it does not mean that the child is nourished. Rice contains a small variety of nutrients such as thiamin, niacin, zinc, and phosphorus. Though important, these nutrients are not enough to support healthy growth and development.128
Before 1975, traditional Cambodian recipes were rich in greens, and gardening was more widespread. This practice and diet were lost to the more basic and sustainable diet of rice and sometimes fish because of the Khmer Rouge and the malnutrition that accompanied it.129 The current mean vegetable consumption rate in Cambodia is 91 g per person per day, while the optimal intake of vegetables is 360 g per person per day.130
Some common practices of food processing in Cambodia that also lead to malnutrition are sun drying, fermentation, and oven drying. These traditional processes remove vital nutrients from foods.131 For example, sun-drying both fruits and vegetables cause the loss of up to 94.2% of vitamin A, and 84.5% of vitamin C.132 Many poor households have little access to vitamin-rich foods; however, the foods they do have are often processed in ways that rid them of their few remaining nutrients. The way that Cambodians traditionally cook and clean their food, specifically fish, reduces micronutrientsVitamins and minerals that the body requires in small amounts and are critical to health. Micronutrient deficiencies can cause a reduction in energy level and mental clarity as well as severe and fatal conditions.7. One study compared the loss of nutrients in fish while sun drying versus oven drying and found that sun drying resulted in the lowest lipid, protein, calcium, and iron content.133 During the cleaning process of a fish, the head is often removed to improve appearance, flavor, and hygiene. However, the head of the fish has the highest concentration of micronutrientsVitamins and minerals that the body requires in small amounts and are critical to health. Micronutrient deficiencies can cause a reduction in energy level and mental clarity as well as severe and fatal conditions.7 such as zinc, calcium, and iron.134 Intakes of nutrients are also reduced by rice consumption because it contains high levels of phytate, an acid that prevents nutrient absorption.135 These cultural beliefs and practices are common throughout Cambodia and greatly impact overall child nutrition in the region.
Food Insecurity
Food insecurity in Cambodia leads to malnutrition as it diminishes the foods that Cambodians eat and results in a lack of dietary diversity, leading to children being stunted, wasted, or underweight. Food insecurity refers to the lack of secure access to enough safe and nutritious food for the growth and development of an active and healthy lifestyle.136 It causes malnutrition because food-insecure individuals are unable to acquire and consume a variety of foods that contain essential nutrientsNutrients that can only be received through consumption.5 and sufficient energy intakeRefers to the total amount of energy consumed through dietary sources, such as carbohydrates, proteins, and fats.3 for healthy growth and development.137 Nearly 40% of children under the age of 5 who live in low-income and middle-income countries are at risk of being malnourished and not reaching their developmental potential.138 Food insecurity is especially prevalent in rural areas. One study showed that in 2015, 25–28% of Cambodians living in rural areas, approximately 4 million people, experienced food insecurity for 2–3 months of the year, with many households experiencing food insecurity for longer periods.139 Another study found that the prevalence of mild, moderate, and severe food insecurity in one region of rural Cambodia was 33%, 37%, and 12%, respectively.140 The average number of children per household studied was 4.6, with an average of 1.23 children under age 5.141 Additionally, children who belong to low and middle-income families are more affected by changes in the cost of high-quality, nutrient-dense food, which is needed to live a healthy life. Over 18% of the population of Cambodia is below the poverty line and makes less than $1.25 per day; thus, it is one of the poorest countries in Southeast Asia.142 Many nutritious foods are available in Cambodia, but because of poverty, the people there are unable to afford them.143
In developing countries, chronic food shortages are common because of political problems, poor growing conditions, and unfavorable harvesting conditions.144 Previous to the Khmer Rouge, rice was attributed to 80% of a Cambodian’s diet. When the country entered a civil war in 1970, crops and land were destroyed.145 By the time the Khmer Rouge seized control in 1975, rice production had dropped by 84% compared to the 1970 harvest.146 The Khmer Rouge also abolished private property rights leaving many rice farmers at risk of losing access to their land for agricultural production. Laws protecting these rights are still fragile and underdeveloped, and studies have shown that the amount of land held by a Cambodian was a determinant of their level of food insecurity.147
The typical Cambodian diet does not meet the needs of most people, particularly children, as they have high nutritional needs that are relative to their energy intakeRefers to the total amount of energy consumed through dietary sources, such as carbohydrates, proteins, and fats.3 and frequent infections.148 Their diet normally consists of rice, consumed at every meal in such quantities that it makes up 60% of the daily energy intake. The remaining part of the diet is fish. Cambodians are one of the populations that eat the most freshwater fish, but many who live in rural areas decide to sell the fish rather than consume it to provide more for their family.149 Even if they reach enough daily energy intakeRefers to the total amount of energy consumed through dietary sources, such as carbohydrates, proteins, and fats.3 through rice and fish consumption, these two foods do not contain all the necessary vitamins and minerals for growth and development. Food insecurity prevents Cambodian children from being able to consume a healthier and more rounded diet that supports their long-term needs.
Enteric Pathogens
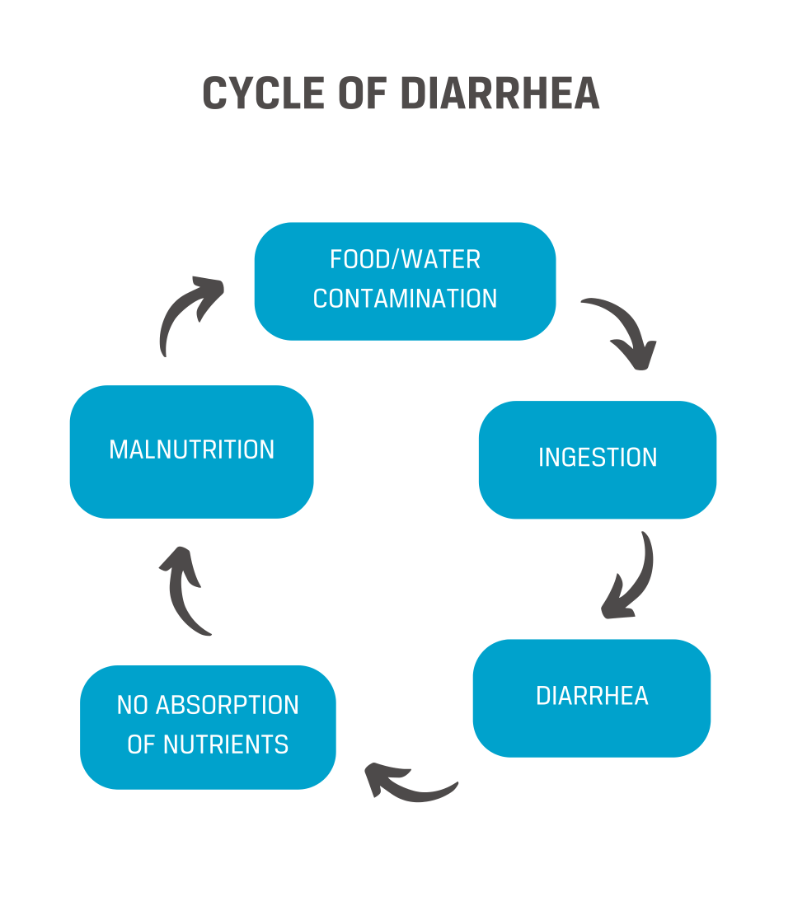
Enteric pathogensBacterias in the intestines of humans and animals that cause diseases.4—bacteria in the stomach and intestine that cause diseases—can lead to malnutrition because they cause many bacterial and viral infections that prevent the absorption of nutrients. These pathogens usually enter the body orally by consuming food or water that has been contaminated with human or animal fecal matter or through direct contact with fecal matter.150 Enteric pathogens include rotavirus, Vibrio cholera, Shigella spp., Salmonella spp., enteropathogenic E. coli (EPEC), and enteroaggregative Escherichia coli (EAEC). These pathogens are typically the cause of severe acute diarrhea, which lasts about 1–2 days.151, 152 However, diarrhea becomes a problem when the illness is persistent, returning after it has gone away. Diarrhea reduces a person’s ability to absorb essential nutrientsNutrients that can only be received through consumption.5 and reach their recommended energy intakeRefers to the total amount of energy consumed through dietary sources, such as carbohydrates, proteins, and fats.3, which leads to malnutrition. Diarrhea infections are most commonly caused by unsafe WASH (water, sanitation, hygiene) practices.153 Research released in 2020 showed that water source and treatment processes were the second leading cause of undernutrition because they led to a variety of enteric pathogensBacterias in the intestines of humans and animals that cause diseases.4. The study found that 15% of stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12 and 21% of wastingWhen children have a low weight-for-height ratio. Wasting indicates malnutrition; children that are wasted have a higher risk of dying from common diseases.13 was due to poor WASH conditions in Cambodia.154 According to this study, there was less access to safe drinking water in the northeastern region of Cambodia, which contributed to higher rates of malnutrition in the area.155
In children under 5, diarrhea is the second-leading cause of death worldwide.156 Diarrhea and malnutrition are frequently seen together because diarrhea causes malnutrition, and malnutrition increases the risk of frequent diarrhea infection.157 Many children who die from diarrhea also die from malnutrition because their bodies do not receive or maintain the necessary nutrients to survive.158 This is because the enteric pathogensBacterias in the intestines of humans and animals that cause diseases.4 that cause bacterial and viral infections, such as diarrhea, prevent nutrients from being absorbed.159 One global study done on diarrheal deaths in children under age 5 determined that 53% of deaths due to diarrhea were also related to malnutrition.160 A multi-country analysis determined that the risk of stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12 increased by 13% on every fifth occurrence of diarrhea before 24 months. This study also found that 25% of stunting occurrences in children under 24 months are related to that child having diarrhea 5 or more times.161 Research done in rural Cambodia and published in 2013 showed that diarrhea was reported in 20.4% of children per visit, resulting in an estimated 5.32 occurrences of diarrhea per child per year (based on 376 children under age 5).162 This means that the average child in Cambodia experiences diarrhea over 10 times in the first 24 months of life, greatly increasing their risk of stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12.163 Another study in Cambodia tested for different types of enteric pathogensBacterias in the intestines of humans and animals that cause diseases.4 in the diarrhea of children under 5 years to determine the cause of pathogens and any existing antibiotic resistance patterns. The pathogens the researchers most commonly found were escherichia coli (20%) and rotavirus (26%).164 Escherichia coli (e-coli) can cause severe stomach cramps, bloody diarrhea, and vomiting; young children with e-coli are at greater risk of developing life-threatening kidney failure.165 In Cambodia, incidences of e-coli have also been associated with faltering child growth.166 Rotavirus, which was also noted as one of the more common pathogens found in the study, causes inflammation in the stomach and intestines, severe diarrhea, vomiting, fever, stomach pain, and dehydration in infants and children.167 Enterotoxigenic E. coli, enteroaggregative E. coli, Shigella, Aeromonas, rotavirus, and adenovirus were also noted among the children with diarrhea.168 The research also discovered that almost 100% of shigella infections were resistant to the treatments provided and that many children with diarrhea were also vomiting and had bloody stools.169 In developing countries, it is normal for children to have more than 3 diarrhea occurrences per year.170 Once again, a high frequency of diarrhea occurrences prohibits the body from being able to absorb the nutrients that are being consumed, thus leading to malnutrition.
Consequences
Anemia
When diets lack essential nutrientsNutrients that can only be received through consumption.5 such as iron, vitamin A, or vitamin B12, malnutrition leads to anemiaA medical condition that occurs when you do not have an adequate supply of healthy red blood cells to carry enough oxygen throughout the body.1 in children. These nutrients would usually be consumed through foods such as meats, fish, beans, and leafy greens, but those are generally absent from Cambodian diets.171 Households that can obtain iron-rich foods do not always benefit from their consumption because the absorption of iron, which is especially important in preventing anemia, is significantly reduced by the consumption of rice, a household staple in Cambodia.172 One study found that consuming 250 mg of phytate, which is contained in rice, reduces the iron absorption rate by 82%.173 A single serving of rice is at least 0.25% phytate (depending on the type of rice being consumed); because a single serving of rice is 146,250 mg, 1 serving of rice contains at least 365 mg of phytate, meaning that high rice consumption in Cambodia leads to decreasing iron absorption and therefore anemiaA medical condition that occurs when you do not have an adequate supply of healthy red blood cells to carry enough oxygen throughout the body.1.174 Anemia is a severe public health problem, and according to research done in Cambodia in 2014, the percentage of anemic children there had not seen significant improvement since 2000.175 In 2014, research in Cambodia showed that children between 6 months and two years old were the most affected by anemiaA medical condition that occurs when you do not have an adequate supply of healthy red blood cells to carry enough oxygen throughout the body.1.176 About 80% of children between 6 and 17 months old suffer from anemia.177 A 2022 study in Cambodia shows that of 1,733 children between 3–5 years, 43.2% (749 children) were anemic.178 Some research has found that iron deficiency may not be the only cause of anemia in Cambodia, but it is the most accepted cause of the medical condition.179
Children with iron deficiency or anemiaA medical condition that occurs when you do not have an adequate supply of healthy red blood cells to carry enough oxygen throughout the body.1 tend to be pale, weak, eat less, and tire easily. They also have a harder time gaining weight, may develop pica, and are more susceptible to frequent respiratory and intestinal infections (such as diarrhea).180 Iron deficiency in children is also associated with impaired cognitive development regarding behavior, cognition, and psychomotor skills. Many countries have found that iron deficiency during critical growth periods may result in irreversible abnormalities.181
Cognitive and Developmental Delays

Malnutrition causes cognitive and developmental delays because it affects brain development and causes impaired mental functioning. Malnutrition affects both the functionality and structure of the brain. The brain of a malnourished child could have tissue damage, growth retardation, disorderly differentiation, a reduction in synapses and synaptic neurotransmitters, and delayed myelination.182 Synapses and synaptic neurotransmitters are vital for life and function. They connect our nervous system, specifically pain or touch, to the brain, helping control motor function and memory formation. A reduction of these can affect the ability to learn and adapt.183 Myelination is also important because it allows more rapid transmission of neural information along neural fibers.184
Children need access to good nutrition starting in the womb to ensure healthy brain development. One recent study done on children under age 12 in Africa and Asia found that malnourished children had lower cognitive function and school achievement.185 Research done in Cambodia found that undernourished children scored poorly on cognitive function, psychomotor development, and fine motor skills tests. The study concluded that malnourished children have lower activity levels and thus interact less with their environment and have fewer opportunities to participate in learning experiences, which results in not developing physical and intellectual skills at a normal rate.186 Another study was done on the island of Mauritius, a country in East Africa with a high prevalence of malnutrition, and was used to determine how malnutrition affects cognitive development. They tested malnourished children at age 3 and then again at 11 years old.187 They found that malnourished children had poorer cognition at both ages, and deficits were stable across the study time. They concluded that children with 3 indicators of malnutrition had a 15.3-point IQ deficit by the age of 11.188 In Cambodia, a developmental milestones chart, a 1-page checkoff chart with expected milestones for each age and group between birth and 8 years, was put into use in 2007–2008. The chart focused on milestones in gross motor, fine motor, language, and social development.189 The use of the charts determined that 25% of children (out of 100) did not reach the milestones in 2007, and 31.5% of children (out of 200) did not reach the milestones in 2008.190 Reaching milestones at the typical age demonstrates that the child is developing as expected. Reaching milestones at an early age is a sign of developmental advancement, while not reaching milestones or reaching them late signals developmental delays.191
Morbidity and Mortality
While morbidityHaving a disease or symptoms of the disease. It can also refer to the amount of a disease within a population. Morbidity also includes medical problems that were caused by a treatment.8 is the existence or symptoms of a disease, mortalityRefers to death or the death of large numbers of people.9 is death caused by a disease. Morbidity and mortality are consequences of malnutrition because malnutrition leads to weakened immune systems, but it is rare that malnutrition is listed as the cause of death in children.192 This is because malnourished children tend to have a higher morbidityHaving a disease or symptoms of the disease. It can also refer to the amount of a disease within a population. Morbidity also includes medical problems that were caused by a treatment.8 rate. Their weakened immune systems contract more diseases and infections, which are then determined to be the cause of premature death.193 Strongyloides stercoralis, also known as threadworm, is one example of increased morbidity in malnourished children in Cambodia. Strongyloides stercoralis is transmitted through contact with soil and can cause long-lasting and potentially fatal infections in immunocompromised children (which includes children with malnutrition who have weakened immune systems).194 The worm automatically replicates inside the child, thus causing recurring infections, each time weakening the immune system further. Common symptoms found during this study were abdominal pain (83.1%), cough (62.5%), epigastric pain (62.3%), diarrhea (60.1%), and urticaria (55.3%).195 The prevalence of Strongyloides stercoralis is greater than 40% among Cambodians.196
According to one study, malnutrition led to 28 infant deaths and 18 neonatalA term referring to newborns, particularly during the first month of life.10 deaths per 1000 live births in Cambodia.197 Projections have shown that Cambodia has 4,454 annual child deaths attributed to malnutrition, which, based on the child mortalityRefers to death or the death of large numbers of people.9 rate in 2020, is nearly one-half of all child mortality in the country.198, 199, 200 Globally, malnutrition contributes to more than 45% of deaths for children under age 5, making it the greatest threat to child survival.201 Between the years 2015 and 2019, malnutrition caused almost half of the total number of child deaths worldwide (5.2 million in 2019).202 The high number of stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12 and wastingWhen children have a low weight-for-height ratio. Wasting indicates malnutrition; children that are wasted have a higher risk of dying from common diseases.13 cases have added to the morbidityHaving a disease or symptoms of the disease. It can also refer to the amount of a disease within a population. Morbidity also includes medical problems that were caused by a treatment.8 and mortalityRefers to death or the death of large numbers of people.9 rates in children under 5 years.203
Practices
Vitamin A Supplementation
Vitamin A supplementation was provided in Cambodia by Helen Keller International (HKI), an organization that supports programs that focus on reducing malnutrition and poor vision.204 Helen Keller International, originally called the British, French, and Belgian Permanent Blind Relief War Fund was first founded in November of 1915 by George and Cora Kessler to help soldiers who were blinded in combat. That same year, the Kesslers asked Helen Keller for her support. After many years and many different names, the name Helen Keller International was adopted in 1977 to demonstrate Helen Keller’s assistance to people who were vulnerable and disadvantaged.205 The current vision of Helen Keller International is to create a world where no one is deprived of the opportunity to live a healthy life and reach their true potential.206 The foundation’s mission is to work with a global community of supporters to help communities striving to overcome long-standing cycles of poverty. They hope to ensure that every person has the opportunity to reach their potential, just as Helen Keller did.207
Helen Keller International works in more than 20 countries across Asia, Africa, and Europe as well as in the United States. They have aided more than 300 million people in the last year with science-based programs that help fight preventable vision loss, malnutrition, and other diseases caused by poverty.208 According to HKI, their vitamin A supplementation program reduces malnutrition by focusing on what they call “hidden hunger”. Hidden hunger (essentially undernutrition) occurs when the body is not getting enough or the right micronutrientsVitamins and minerals that the body requires in small amounts and are critical to health. Micronutrient deficiencies can cause a reduction in energy level and mental clarity as well as severe and fatal conditions.7 to grow and fight diseases.209 HKI specifically targets malnutrition in women, infants, and young children.

The foundation works to supplement children between the ages of 6 months and 5 years with a vitamin A capsule every 6 months by means of healthcare workers or community volunteers.210 They deliver micronutrient supplementation, specifically vitamin A and iron, to these groups in the areas where they work, as well as train healthcare workers to counsel families on nutrition.211 GiveWell listed HKI’s vitamin A supplementation program as one of their top-rated charities in a review of the program carried out in Sub-Saharan Africa.212 GiveWell has also investigated the effectiveness of the program in Sub-Saharan Africa and found that support from HKI was necessary for supplementation to occur.213 In Cambodia, the vitamin A supplementation program started small but grew over time and was successful. Eventually, Helen Keller International convinced the Cambodian government to take over the program and increase its scale through national policies. One such policy is the National Vitamin A Policy which was adopted in 1994 by the Cambodian Ministry of Health, which gave supplements on established national and sub-national immunization days.214, 215 Both GiveWell and The Life You Can Save have stated that HKI’s supplementation program is cost-effective, far-reaching, and transparent.216, 217
Impact
According to The Life You Can Save, vitamin A supplementation costs $1.23 per supplement and can reduce child mortalityRefers to death or the death of large numbers of people.9 by 12–24%.218 Vitamin A deficiency, which contributes to malnutrition, has high rates in South Asia. Trials conducted in South Asia show that there was a significant reduction (21%) in mortality during the first 6 months of life after receiving vitamin A supplementation.219 The trials also reported a reduction of maternal mortalityRefers to death or the death of large numbers of people.9 rates by 40% when following routine dietary supplementation during pregnancy.220 A 2021 study, which tested the effectiveness of vitamin A supplementation programs in 51 different countries, found that just under 4 in 5 children were receiving adequate vitamin A in their diet.221 The Cambodian Ministry of Health stated that vitamin A supplementation reduced diarrheal occurrences by 40% and mortality by 23% in children aged 6 months to 5 years.222 Other researchers who tested the coverage of vitamin A supplementation in Cambodia in 2008 found that 42.8% of preschool-aged children (ages 1–5) received vitamin A supplementation within the previous 6 months.223

Gaps
Even though sources say that Helen Keller International is transparent, data regarding their vitamin A supplementation program in Cambodia is not available or discoverable on their website. Furthermore, data on the effectiveness of vitamin A supplementation as a whole is limited. Researchers debate about whether a daily low dose or semi-annual high dose of vitamin A is more effective.224 There is also the worry of the possible side effects of a higher dose, and researchers wonder if a higher dose is as effective.225, 226 More testing is required to verify the effectiveness and sustainability of the practice, especially in terms of stuntingRefers to low height compared to age;11 impaired growth and development experienced by children resulting from poor nutrition, repeated infection, and inadequate psychosocial stimulation.12, wastingWhen children have a low weight-for-height ratio. Wasting indicates malnutrition; children that are wasted have a higher risk of dying from common diseases.13, and underweight. Some practices have been evaluated, but data about the efficacy of vitamin A supplementation are not recent, and most studies occur in Africa rather than Asia. Program coverage also appears to be an issue. While national surveys were conducted in 2000 and 2014, no data on vitamin A was collected, making it difficult to understand the impact of the micronutrient intervention.227
Preferred Citation: Bernal, Ashley Girvin. “Child Malnutrition in Cambodia.” Ballard Brief. October 2022. www.ballardbrief.byu.edu.
Viewpoints published by Ballard Brief are not necessarily endorsed by BYU or The Church of Jesus Christ of Latter-day Saints